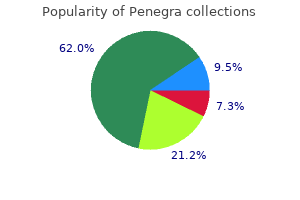
"Quality 50 mg penegra, mens health shoulder workout".
By: U. Gembak, M.A., Ph.D.
Professor, Roseman University of Health Sciences
Ultrasound is the easiest way of making the diagnosis prostate massagers for medical purposes purchase online penegra, and aids in liver aspiration prostate oncology specialists generic penegra 50mg with amex. Until cultures are available mens health workout programs effective 50 mg penegra, use broad spectrum antibiotics: metronidazole, gentamicin, cloxacillin and ampicillin. Try to aspirate the abscess completely; if you fail, proceed to open drainage (as above). Test for sickle cell disease and schistosomiasis, if these are common in your area. The geographical distribution of the hepatitis B virus, based on incidence of HbsAg in blood samples, correlates with hepatoma incidence. Typically, the pain is made much worse by alcohol; so much so that it may have caused abstinence. Usually, presentation is late with a large, or even a huge, firm, irregular, tender liver. Quite a small tumour may cause prostration but normal activity may continue with a large tumour. Look for collateral veins running vertically over the anterior costal margin, or parallel to the spinous processes. Listen over the tumour for a bruit or friction rub; this may be intermittent, so listen on several occasions. Try to distinguish those you can treat, such as liver abscesses, hydatid cysts, and tuberculosis, from those you can only palliate. The best and most non-invasive tool by far is an ultrasound: do all you can to get such a machine and get acquainted with it (38. If you cannot get histology, aspiration with a fine needle may still be useful to detect pus or tuberculosis. Though this test is unlikely to be available locally, it may be easier to get a laboratory to do it rather than get histology on a potentially dangerous liver biopsy. Blood-stained fluid supports the diagnosis of malignancy, not necessarily of the liver. This has a sharp stout end (a), with an adjustable guard (b), and a Luer lock (c). B, viewed in cross section, the assembly has an obturator outside the needle, and a blocking pin, which slips loosely inside the needle and prevents the biopsy fragment from falling back, and breaking up in the syringe. To take a biopsy using a Menghini needle: (1) insert it through the skin, (2) expel skin fragments, (3) aspirate, (4) advance the needle into the liver, with the patient holding his breath, and gently suck up tissue by holding the syringe steady, (5) extract the needle whilst gently maintaining suction. Pass the needle point through the anaesthetized track through the intercostal space. Start to aspirate, and while continuing to aspirate, rapidly push the needle into the liver perpendicular to the skin, then, immediately pull it out again. Continue aspirating until you have placed the needle point under some saline in a glass dish. With firm, but well-controlled pressure, push the needle through the abdominal wall while the patient holds his breath. If the needle moves with respiration, its tip is already in the liver; if not, ask him to hold his breath again, and gently push it 3cm further in, or until it moves. The inner jaws grasp a core of tissue, after which you slide the sleeve over them to trap it. Its disadvantage is that it is less likely to withdraw a satisfactory specimen in a cirrhotic. Ask him to hold his breath, then remove the inner obturator and replace it with the biopsy jaws. Steady the needle with your left hand, and push the jaws with your right hand into the needle as far as they will go. Hold the biopsy jaws firmly with your right hand, and slide the outer jaws 3cm further into the liver.
Melanotan-Ii. Penegra.
- Dosing considerations for Melanotan-ii.
- Prevention of sunlight-induced skin cancers and other conditions.
- Are there safety concerns?
- What is Melanotan-ii?
- How does Melanotan-ii work?
- What other names is Melanotan-ii known by?
- Use by injection to produce erections in men with erectile problems.
- Use by injection to produce tanning of the skin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96852
Pelvic floor electrical stimulation for the treatment of urge and mixed urinary incontinence in women prostate 64 liquid protein order penegra 50 mg on line. American Society for Colposcopy and Cervical Pathology - Medical Specialty Society; 2005 man health daily shopping category cheap 100mg penegra with visa. A prospective randomized study comparing acupuncture with physiotherapy for low-back and pelvic pain in pregnancy prostate cancer 911 doctor samadi purchase penegra 50 mg on-line. Physical therapist Management of Chronic Prostatitis/Chronic Pelvic Pain Syndrome. Wrist and proximal finger joints are frequently affected; however, the neck, jaw, and all extremity joints can be involved. Chronic inflammation leads to joint destruction with instability and loss of range of motion. The severity of stiffness may better differentiate a primary inflammatory process from other joint processes. With normal sleep patterns, stiffness is most pronounced in the morning, in part due to redistribution of interstitial fluid while sleeping. Swollen joints with an applied load or joints with rapidly evolving effusions may be extremely painful due to high intra-articular pressures that lead to excessive stresses on the extensively innervated periarticular supporting structures. Possible Consequence or Cause Fracture, ligament tear Infection Neuropathy Deep vein thrombosis Cause of symptoms (metastatic or primary) Arterial occlusion Infection Red Flag Severe trauma Fever, severe pain Diabetes Unilateral edema Cancer Discoloration of extremity Immune-compromised state Presentation Patients may present with stiffness, and tenderness of affected joints. Enlargement of synovial membrane and deformity of the joint may develop over time as articular and supporting structures are damaged by the inflammatory process. The patient may also present with limitation of motion, generalized malaise and fatigue. Subjective Findings Complaints of joint stiffness after sleep or periods of inactivity Pain, redness, swollen and warm joints Multiple joint complaints, frequently symmetrical Fatigue Fever Possible weight loss Objective Findings Objective findings may include: Scope of Examination Examine the musculoskeletal system for possible causes or contributing factors to the complaint. Inspection Nodules Joint swelling Symmetrical involvement Deformities Palpation of bony and soft tissue Joint tenderness 52 of 937 Referral Guidelines Refer patient to their primary care provider for evaluation of alternative treatment options if: Improvement does not meet above guidelines, or improvement has reached a plateau Atrophy of extremity occurs Neurologic testing worsens Range of motion plateaus or decreases Management/Intervention Use of modalities and/or passive treatments should be limited. Hind foot pronation is addressed with custom inserts Knee orthosis to control patellar alignment and hyperextension Dynamic hand splints are used to increase dexterity. Resting hand splints are used for acutely inflamed joints © 2017 eviCore healthcare. In most cases, this type of care is largely active and is typically directed by the provider and performed by the patient as a home program. Expected Outcome Decrease pain and stiffness Procedures/Modalities Such As Superficial or deep heat i. Knee orthosis to control patellar alignment and hyperextension Dynamic hand splints are used to increase dexterity Decrease stiffness and Active range of motion improve flexibility Stretching exercises within pain free range Joint mobilization © 2017 eviCore healthcare. American Physical Therapy Practice, Interactive Guide to Physical Therapist Practice, 2nd Edition, 2003. Ottawa Panel Evidence-Based Clinical Practice Guidelines for Therapeutic Exercises in the Management of Rheumatoid Arthritis in Adults. Therefore, urgency and frequency (overactive bladder) are dysuria, not incontinence. There are several types of incontinence: Stress Urinary Incontinence Involuntary leakage of urine with increased intra-abdominal pressure, i. In the elderly, it may result from rolling over in bed, sitting up from reclining, or getting up from a chair. In a younger population, running, bending over, lifting, and jumping are common activities which lead to stress urinary incontinence. Most often it is associated with an incompetent bladder neck and sphincter, weakened urethral musculature, and following multiple vaginal deliveries or pelvic surgery. Stress urinary incontinence results in smaller amounts of urine loss rather than a total loss of urine in one accident.
We will not discuss drug- or allergy-mediated myocarditis or myocardial damage related to prostate doctor cheap 50mg penegra ischemic heart disease androgen hormone 15 order penegra with a visa. Myocarditis the major features of myocarditis are disturbances in heart rhythms mens health fat burning workout buy 50 mg penegra with mastercard, congestive heart failure, or cardiogenic shock. None of the clinical features described are diagnostic for myocarditis, and until the use of the endomyocardial biotome, the diagnosis could only be established with certainty by postmortem examination. The reasons for this wide discrepancy may be related to exposure to the different types and strains of cardiotropic viruses as well as genetic differences in host populations. Many patients recover spontaneously inter supportive treatment but the five-year survival of biopsy-proven giant cell myocarditis is only 56 percent, and in pediatric patients, the mortality rates may be even higher. Patients may also display signs or symptoms of arrhythmias, systemic pulmonary vein congestion, triple gallup rhythms, and mitral or tricuspid regurgitation. Once the diagnosis is established, the outcome is poor, with a five-year mortality of 46 percent. Some reports have indicated that there is a relationship between the two, but biopsies in both diseases are needed to prove or disprove this concept. In addition, Coxsackie virus Bspecific nucleic acid sequences have been found in the heart tissues of a small number of these patients. The clinical spectrum varies from asymptomatic 222 Autoimmune Considerations As in other immune-mediated diseases of the heart, many investigators have now Immunological Aspects of Cardiac Disease explored the role of autoantibodies to the heart as an explanation for the disease. Using cardiac tissue from rats and humans (either frozen tissue or isolated myocytes), immunofluorescence studies showed the antibody localized on the myocyte, giving a sarcolemmal, myolemnal pattern or on the striations, producing a fibrillar pattern. Whether these two patterns represent different forms of the disease is unclear because both patterns were seen in the sera of mice immunized with cardiac myosin. The specificity of these patterns is unclear because many normal sera gave the same pattern in one series (91 percent of patients vs. Another series was more specific where 59 percent of acute myocarditis patients where positive versus 0 percent of healthy controls. Here 97 of 103 samples exhibited positive reactivity but no single pattern was seen to be unique in either group. However, myocarditis sera reacted more to myosin heavy chain, while cardiomyopathy sera reacted more to muscle actin. Large-scale evaluation is necessary before one can conclude that the detection of any single antibody, or group of antibodies, is sufficiently sensitive and specific to replace the endomyocardial biopsy as a primary diagnostic tool. None of these antibodies to cardiac antigens is known to play a direct pathogenetic role in the disease. It is not clear, however, whether these antibodies have access to their target antigens in vivo. In this respect, myocarditis differs from most autoimmune diseases, which predominantly affect females. Acute myocarditis is associated with infections of many types, including bacterial, rickettsial, viral, mycotic, protozoan, and helminthic. As stated previously, several viruses have been implicated in this disease and, in some cases, multiple viruses may be detected in the heart. In Europe and North America, among the most common agents are the enteroviruses and the adenoviruses. It has been reported that Coxsackie virus group B infections were associated with at least half of the acute cases of myocarditits and by immunofluorescence, the Coxsackie virus B antigen was found in the myocardium of 30. Although infections with Cox Sackie Virus B3 are relatively common in humans, the development of clinically significant cardiac disease in humans is uncommon, suggesting that differences in host response may be crucial. These differences may be related to genetic factors or may relate to virus-specific receptors on host tissue. The disease reached its peak on day 7 and gradually resolved, so that by twenty-one days after infection the heart was histologically normal. The first phase occurred during the first week after infection and was characterized by focal necrosis of myocytes and an accompanying focal acute inflammatory response with a mixed-cell infiltrate, consisting of polymorphonuclear and mononuclear cells.
Infection spreads up and down a muscle prostate oncology quizzes purchase penegra 50mg fast delivery, and has less tendency to prostate gland histology buy penegra 100 mg amex spread from one muscle to prostate cancer 04 buy penegra on line another. As infection progresses along a muscle, it changes from brick red to purplish black (6-17). At first the wound is relatively dry; later, you can express from its edges a thin exudate with droplets of fat and gas bubbles, which becomes increasingly offensive. Try to prevent gas gangrene: (1);Always perform a thorough wound toilet, especially in all extensive muscle wounds of the buttock, thigh, calf, axilla or retroperitoneal tissues. There is probably no absolute need for prophylactic antitoxin serum, which is probably hard to obtain, if you have performed a thorough wound debridement. Once gas gangrene has developed, do not delay exploring the wound because there is hypotension. B, as the infection advances down muscle, its colour changes from its normal purple, through brick red and olive green, to purplish black. Both require drainage and penicillin or doxycycline but neither needs radical muscle excision. When you remove the affected tissue, the muscle underneath appears healthy, and bleeds and contracts normally. Suggesting anaerobic streptococcal myositis: Spreading redness and swelling originating in a stinking discharging wound with Gram+ve cocci and pus cells in its exudate. The muscles are boggy and pale at first, then bright red and later pale and friable. Make radical incisions through the deep fascia to relieve tension and provide drainage. Although clostridia are not sensitive to metronidazole, some other anaerobic bacteria are and may co-exist in the wound, so use it. Open the wound, enlarge it if necessary, lengthwise in the limb, and cut the deep fascia throughout the whole length of the skin incision. If necessary, remove whole muscles from their origin to insertion, part of a large muscle, or a whole group of muscles. Close the stump by delayed primary suture, even if you think you are amputating through healthy tissue. Expect, and treat as best you can, the dehydration, vomiting, delirium, jaundice, and anuria that may develop. This followed an intramuscular injection, but it could equally well have followed a severely contaminated wound. One or more muscles become exquisitely painful, tender, and swollen, and the skin overlying smooth and shining. A single muscle may be involved, or a group of them, or several in different parts of the body. Later, the signs of inflammation may subside as the infected muscle is replaced by pus and becomes fluctuant. The patient is very ill and drowsy, with a high fever, and multiple tender areas over the muscles. The condition rapidly progresses, so that he becomes desperately ill with a swinging fever, weakness, prostration, dehydration and hypotension. Pyaemia associated with pyomyositis results in a sequence of abscesses in one muscle after another. C, the distinction between pus in the muscles (as in pyomyositis), and pus between them, as in an abscess round a dead Guinea worm (34. If you are not sure where to point your needle, use an ultrasound to guide you if possible. If it is large, extend the incision, so that you can insert your finger, break down any loculi and explore the whole cavity. If the bone feels rough and craggy at the bottom of the abscess cavity, it may be involved; if so, this is osteomyelitis, not pyomyositis. If there is already coma from septicaemia, do not add to the problems by using an anaesthetic! The exact site of the tenderness and swelling will usually lead you to the correct diagnosis. There are several other possibilities which depend on the site of the abscess: In the upper abdomen, pyonephrosis or a perinephric abscess (6. If there are very many or very severe lesions, you may have to make >10 incisions, with repeated staged visits to the theatre, to evacuate pus and remove dead muscle.